32 Iris Repair
32.1 Pupilloplasty
5. Pupilloplasty
Iris defects may be congenital (iris coloboma) or occur secondary to trauma (iatrogenic or accidental). Repair of these may be required if there is symptomatic monocular diplopia or photophobia. Vitrectomy (anterior or posterior) should be performed to ensure that all vitreous has been cleared from the pupillary plane and behind the iris prior to iris repair.
One method of repairing an iris defect is to use a Siepser knot. This slip knot can be tied outside of the eye. It can be used to close iris defects or fixate subluxed IOLs. The technique below is a modified technique described by Osher et al.[1]
- Create a wide clear corneal paracentesis adjacent to one edge of the iris defect
- Introduce a 10-0 Prolene suture with a long curved needle through the paracentesis, across the iris defect (anterior to posterior at the proximal side, posterior to anterior at the distal side) and out through clear cornea opposite to the paracentesis
- Using a Kuglen hook, retrieve a loop of suture from between the distal iris defect and where the needle exited on the opposite side. Pull this loop out the proximal paracentesis
- From the loop of externalised suture, identify the side which is closest to the iris defect. Tie the proximal (free) end of the suture over this twice. This creates a slip knot
- Pull the two free ends of the suture to allow the slip knot to enter the eye and close the iris defect
- Repeat step 3. Using a Kuglen hook, retrieve a loop of suture from between the distal iris defect and where the needle exited on the opposite side. Pull this loop out the proximal paracentesis
- From the loop of externalised suture, identify the side which is closest to the iris defect. Tie the proximal (free) end of the suture under this twice. This is a locking throw that ensures that the slip knot won’t unravel
- Pull the two free ends of the suture to allow the slip knot to enter the eye and close the iris defect
- More than one Siepser knot may be required to close an iris defect
Osher RH, Snyder ME, Cionni RJ. Modification of the Siepser Slip-knot Technique. JCRS 2005;31(6):1098- 100.
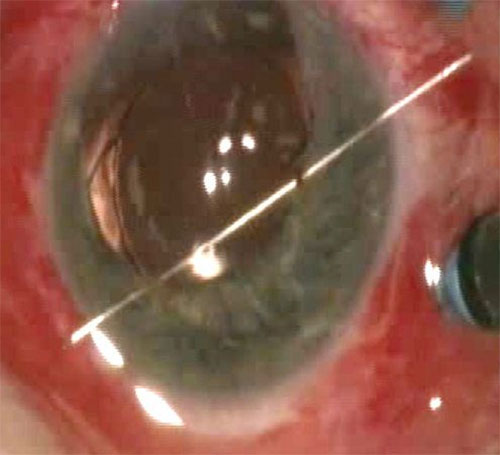
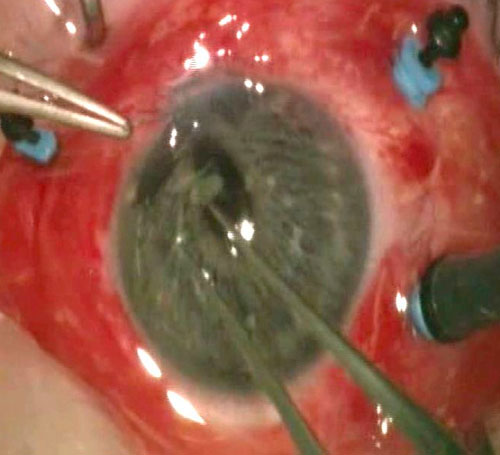
Figure 31.2 Pupilloplasty
In this case a 10-0 Prolene* suture with a long straight needle has been used. If available, a long curved needle is often easier to use for the purposes of pupilloplasty.
All rights reserved. No part of this publication which includes all images and diagrams may be reproduced, distributed, or transmitted in any form or by any means, including photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the authors, except in the case of brief quotations embodied in critical reviews and certain other noncommercial uses permitted by copyright law.
Westmead Eye Manual
This invaluable open-source textbook for eye care professionals summarises the steps ophthalmologists need to perform when examining a patient.